Sensorineural hearing loss
Authors: Diane Lazard
Contributors: Benjamin Chaix, Frédéric Venail, Sam Irving
Strictly speaking, sensorineural hearing loss concerns pathology of the hair cells and neurons. Nevertheless, from a clinical point of view, sensorineural hearing loss is sometimes classified as perceptual, despite this term being ambiguous because most hearing loss occurs in the cochlea. It is therefore worth pointing out that not all perceptual hearing loss is sensorineural.
Note – the following pages concern either clinical aspects of hearing loss, or experimental results that describe the pathophysiological and molecular mechanisms that cause it.
.
Etiology
There are three main causes of acquired sensorineural hearing loss: ototoxic drugs (ototoxicity); overstimulation (acoustic trauma); and age (presbycusis). A fourth related cause is excitotoxicity, one of the main components of acoustic trauma, which is also involved in ototoxicity and some sudden hearing losses.
Symptoms:
Sensorineural hearing loss is not painful (with the exception of acute acoustic trauma, which is addressed in a seperate chapter). Headache can, however, be a sign of advanced tumour when associated with:
– Decrease in hearing acuity
– Dizziness
– Tinnitus
– Facial paralysis
Clinical examination
Outer and middle ears are normal. The tympanogram is also normal.
A thorough examination of the cranial nerves is essential (facial nerve in particular for vestibular function, although all facial nerves should be tested if any doubt exists), as well as a neurological examination.
Characteristic audiometry and acoumetry are presented below.
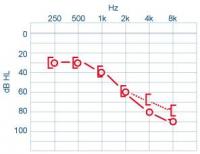
– Weber results lateralised on the healthy side in the case of unilateral problem, or on the side with the least hearing loss in the case of assymetry.
– Rinne: Air conduction > bone conduction
– Reduction of air and bone conduction with similar curves (see image).
– Stapedial reflex: variable, depending on etiology (see endocochlear/retrocochlear hearing loss)
– Speech: shifted to the right and can reach 100% at higher intensities. The usual sinusoidal is often altered. It is also common to observe a decrease in comprehension with an increase in intensity (decreased intelligibility at high intensities). A common complaint is “I can hear you, but I don’t understand”.
Les oreilles externe et moyenne sont normales. Le Tympanogramme est normal.
L’examen attentif des paires crâniennes est primordial (nerf facial, examen vestibulaire en particulier mais toutes les paires crâniennes doivent être évaluées au moindre doute), ainsi que si nécessaire un examen neurologique.
Endocochlear hearing loss
At around 80dB, a stapedial reflex can be detected as it is recruited. Acoustic evoked potentials have normal latencies but decreased thresholds.
Etiology can involve: presbycusis, congenital deafness with cochlear origins, Meniere’s disease and sudden hearing loss. All these factors have their own chapter on this site for your information.
Generally, presbycusis is bilateral and symmetrical. The other etiologies can be unilateral or bilateral but asymmetrical or have different onset times.
Retrocochlear hearing loss caused by a tumour on the vestibulocochlear nerve.
The stapedial reflex appears with a stimulus intensity greater than 80 dB, but is absent in the case of substantial hearing loss. Auditory evoked potentials exhibit decreased thresholds and abnormal latencies (increased interval between waves I and V).
The most common tumour of the vestibulocochlear nerve is vestibular schwannoma (or acoustic neuroma):
– benign tumour of the inferior vestibular nerve which develops in the internal auditory canal towards the cerebellopontine angle.
– there is a risk that it can compress other structures: the Vth crantial nerve, brainstem and cerebellum.
– It does, however, generally exhibit slow growth (1mm to 1cm/year) and low frequency 1/100000.
Clincal signs:
– Unilateral perceptual hearing loss (sudden or progressive): 70%
– Unilateral tinnitus: 10%
– Dizziness: 10%
– More rarely: neurological symptoms (V, VII, migranes, cerebellar symptoms).
Specific complementary tests:
– Pure tone and speech audiometry: tonal-vocal discordance = greater intelligibility difficulties than for pure-tone audiometry alone
– Vestibular examination: hypofunction
– Radiological examination: MRI with injection of contrast agent.
Treatment:
– Monitoring
– Surgery
– Radiotherapy